Virtual diabetes care models can successfully support those living with either type 1 or type 2 diabetes (T1D or T2D) through integration of continuous glucose monitoring (CGM) devices for self-management of diabetes. In the Virtual Diabetes Specialty Clinic (VDiSC) study model which included CGM device use plus remotely delivered comprehensive diabetes education, care, and behavioral support, 99% agreed that CGM helped them manage their diabetes, whether they had type 1 or type 2. A total of 78% of participants with T1D and 90% of participants with T2D said that they changed their eating habits based on their CGM data.
Among T1D participants, mean HbA1c levels reduced from 7.8% to 7.1% from baseline at three months, and 7.1% at six months. The average time in range for glucose (TIR) values to 180 mg/dL increased 11% over six months. Similarly, in T2D participants, mean HbA1c reduced from 8.1% to 7.1% from baseline to three months, and 7.1% at six months, with an 18% TIR increase over six months.
In T1D patients, the average percentage of TIR values less than 70 mg/dL decreased by 0.8% over six months, and the average percentage of TIR values less than 54 mg/dL decreased by 0.3% over six months. In the T2D group, hypoglycemia was rare, with a mean percentage of TIR values of less than 70 mg/dL and 54 mg/dL in 0.5% and 0.07%, respectively, over six months.
These findings were reported in “Comprehensive Telehealth Model to Support Diabetes Self-Management” by Grazia Aleppo, M.D.; Robin L. Gal, MSPH; Dan Raghinaru, MS; and colleagues. The researchers recruited participants from the CVS Health Clinical Trial Services, endocrinology clinic referrals, and primary care centers in the United States between August 24, 2020, and May 26, 2022. A total of 234 individuals (160 had type 1 diabetes and 74 had type 2 diabetes) participated in the study. Study follow-up lasted for a minimum of 26 weeks. The goal was to evaluate a virtual clinic model that could facilitate comprehensive diabetes care, support CGM integration into diabetes self-management, and provide behavioral health support for diabetes-related issues. A team of providers from Cecilia Health provided virtual clinic support for the VDiSC study.
For more information, contact: Robin L. Gal, MSPH, Director of Research Operations, Jaeb Center for Health Research, 15310 Amberly Drive, Suite 350, Tampa, Florida 33647; Email: rgal@jaeb.org; Website: http://www.jaeb.com/
This presentation took place at The 2023 OPEN MINDS Strategy & Innovation Institute. Dr. Doug Wright, Chief Operations Officer, Southeast Kansas Mental Health Center, Shawna Wright, Ph.D., LP, Director KU Center For Telemedicine & Telehealth, University of Kansas Center For Telemedicine & Telehealth, and Sharon Hicks, Senior Associate for OPEN MINDS explored:
Building hybrid service delivery systems, policies, and procedures
Training and development of staff members to be hybrid proficient
Using technology to optimize hybrid delivery systems
During 2022, 38% of consumers preferred virtual behavioral health services to in-person services, based on more than 8,000 responses to the Rock Health 2022 Digital Health Consumer Adoption Survey. Most consumers preferred telehealth visits for prescription refills (61%), and the preference for telehealth was even higher among consumers with multiple prescriptions, at 64% among those with one-to-three prescriptions and 71% among those with four or more prescriptions.
More than half of consumers (51%) preferred telehealth for minor illness consultations, and 23% preferred telehealth for emergency care. Only 27% preferred telehealth for annual wellness visits. Among people with chronic health conditions, 35% said they preferred telehealth visits. The lowest level of interest was for virtual physical therapy: only 20% preferred virtual sessions.
About 80% of the survey respondents said they had used telehealth at some point in their lives, up from 72% in the 2021 survey. The use of telehealth increased more than 10 percentage points between 2021 and 2022 among three groups:
Rural: 73% said they used telehealth, up from 60%.
Uninsured: 50% said they used telehealth, up from 37%.
Older adults (age 55+): 76% said they used telehealth, up from 64%.
These statistics were reported in “Consumer Adoption Of Digital Health In 2022: Moving At The Speed Of Trust” by Madelyn Knowles, Adriana Krasniansky, Ashwini Nagappan, and colleagues at the Stanford Medicine Center for Digital Health. The authors analyzed responses to the Rock Health 2022 Digital Health Consumer Adoption Survey. The online survey has been conducted annually since 2015 to monitor trends in consumer attitudes toward and behaviors surrounding digital health. The 2022 survey was conducted from July 12 to August 22, 2022, with a nationally representative sample of 8,014 adults.
For more information, contact: Rebekah Williams, Lead, External Relations, Rock Health, 301 Howard Street, San Francisco, California 94105; Email: Rebekah@rockhealth.com; Website: https://rockhealth.com/
US Acute Care Solutions (USACS), the largest physician-owned acute care practice in the nation, and Array Behavioral Care, the nation’s leading virtual psychiatry and therapy practice, announced a strategic partnership to offer comprehensive acute medical and psychiatric care services to health systems. With the newly formed Behavioral Emergency Stabilization and Treatment (BEST) model, USACS and Array will unite their clinical and technological expertise to combat the growing epidemic of acute mental illness that has impacted the nation for decades.
The downstream result of delays in acute psychiatric care has a domino effect on non-psychiatric consumer care and throughput. Array’s sophisticated virtual psychiatric care platform and clinical expertise can improve the speed of evaluation, treatment initiation and patient throughput, which improves the quality of care for all patients in the acute care space. Additionally, by using virtual technology, Array and USACS will be able to facilitate quicker access to care and further address social determinants of health.
Founded by emergency medicine and hospitalist physicians across the country, USACS is solely owned by its physicians and hospital system partners. The group is a national leader in integrated acute care, including emergency medicine, hospitalist, and critical care services. USACS provides high-quality care to approximately nine million consumers annually across more than 500 programs and is aligned with many of the leading health systems in the country.
Array Behavioral Care is the nation’s leading clinician-centric virtual psychiatry and therapy practice with a mission to transform access to quality, timely behavioral health care. Array offers telepsychiatry solutions and services across the continuum of care, from hospital to home, through its OnDemand, Scheduled and AtHome divisions. For more than 20 years, Array has partnered with hundreds of hospitals and health systems, community health care organizations and payers of all sizes to expand access to care and improve outcomes for underserved individuals, facilities, and communities. As an industry pioneer and established thought leader, Array has helped shape the field, define the standard of care and advocate for improved telepsychiatry-friendly regulations.
In the proposed Medicare physician fee schedule for calendar year 2024, the Centers for Medicare & Medicaid Services (CMS) proposed extending the Medicare Diabetes Prevention Program (MDPP) for four years, and telehealth flexibilities for this program. During the COVID-19 public health emergency (which started in March 2020 and ended on April 11, 2023), CMS permitted telehealth services to replace the MDPP in-person service requirements. Currently, MDPP suppliers are required to resume in-person delivery of the MDPP set of services after December 31, 2023. Under this proposal, MDPP services could be provided via telehealth through December 31, 2027.
The proposed extension affects the following policies:
Permitting alternatives to the requirement for in-person weight measurement for participant baseline weight and any weight loss-based performance goals. These alternatives include using a scale that transmits weight securely via wireless or cellular transmission or by patient self-reporting via a date-stamped photo or video recording of the scale.
Eliminating the maximum number of virtual services that MDPP suppliers can provide, so long as the virtual services: are furnished in a manner that is consistent with the Centers for Disease Control and Prevention (CDC) Diabetes Prevention Recognition Program (DPRP) standards for distance learning sessions follow the CDC-approved National DPP curriculum requirements, and are facilitated by a supplier that has an in-person DPRP organizational code.
CMS proposed amending the MDPP fee schedule to allow for fee-for-service (FFS) payments for beneficiary attendance during the core services period. The proposed FFS payment, at $25 per session, would apply when an MDPP participant attends a core session during the first six months or a core maintenance session during months 7 to 12. CMS proposed allowing up to 22 sessions over a 12-month period in which time the participant will attend in-person or distance learning session every week, for a maximum of 16 sessions. In the following six months, the participant likewise attends one in-person or distance learning session each month, for a maximum of six sessions.
The proposal retains the performance-based payments for diabetes risk reduction, which are measured in terms of weight loss. For performance payments, the MDPP supplier is eligible for a $145 performance payment for each of their MDPP participants who achieves 5% weight loss, and another $25 performance payment if the participant achieves 9% weight loss. The supplier is also eligible for another performance payment of $8 if the beneficiary maintains the weight loss during the core maintenance sessions during months 7 to 12.
This presentation, sponsored by Qualifacts, took place at The 2023 OPEN MINDS Executive Leadership Retreat. Paul Duck, Chief Strategy Officer, and Carol Clayton, Ph.D., Senior Associate for OPEN MINDS, discussed a road map for digital-first evolution and what it means to be a digital-first organization, the eight dimensions of a digital-first framework for quality and performance, and critical organizational competencies needed for leading-edge technology transformation. The session includes Nicholas Chepesiuk, Vice President, Virtual Care & Innovation, Qualifacts spoke on how to optimize your virtual care model including interoperability with existing systems, decreasing workload with automation, and increasing patient engagement.
Autism prevalence rates are on the rise. The latest numbers for children identified with autism spectrum disorder (ASD) are up 22% from 1 in 44 in 2018, to 1 in 36 in 2020—and 317% since 2000 (see Autism Prevalence Increased 22% From 2018 To 2020).
Like many areas of health care, one solution to addressing access issues is to leverage the power of technology. And in our recent Circle Executive Roundtable, Harnessing The Power Of Virtual Autism Evaluations: The As You Are & Autism Analytica Case Study, Steven Hicks, M.D., Ph.D., the Chief Medical Officer of As You Are and Mirko Uljarević, M.D., Ph.D., Clinical Assistant Professor in the Department of Psychiatry and Behavioral Sciences at Stanford University, provided a look at the emerging use of technology to expand access to autism diagnostic services.
As You Are is a telehealth service focused on autism diagnosis for children starting at 16 months of age. The company launched in 2022 and currently operates in nine states. The As You Are physician network provides diagnostic services through a pediatric, virtual care, telehealth clinic. This service is provided both directly to parents and guardians by board certified pediatricians who use standardized assessment tools to observe a child’s behavior in the comfort of their own home. Once an autism diagnosis is made, As You Are connects the family to appropriate services and provides ongoing support. Medicaid makes up the majority of their payments (63%), although commercial insurance is also accepted
As part of its model, the As You Are team uses tools provided in a unique software platform to support clinical screening, pediatric evaluation and diagnosis, and care coordination. Clinicians are also able to send Autism Analytica’s Virtual assessments directly to parents to explore medical comorbidities and alternative diagnoses. Virtual and enable remote collection of a comprehensive set of caregiver reported measures, capturing the full clinical and cognitive profile of the child. As You Are physicians review the results with the family, explain how they determined their diagnosis, and provide recommendations for therapy and intervention. The diagnostic data is made available to the family and the child’s caregivers for use with pre-authorization of services. Importantly, the Autism Analytica assessment platform provides crucial information for selecting appropriate treatment targets for each child and assists clinicians in being able to accurately monitor treatment-related changes.
When looking at technologies to support diagnosis and treatment for this population, Dr. Uljarević identified four issues facing children with autism and their families: delayed diagnosis, lengthy wait times, a shortage of subspecialists, and a lack of objective measures.
He said, “Firstly, there is a delay in diagnosis, due in large part to the time-consuming evaluation process and a lack of qualified providers who are comfortable diagnosing. The second problem is lengthy wait times. Families must wait, on average, at least six to 12 months from referral to the actual receipt of the diagnosis. The third issue is a severe shortage of subspecialists who can work effectively with kids with autism and their families. Finally, one of the root causes of all these problems is the lack of objective measures. Those that are available provide only partial indicators of the child’s behavior, behavioral profile, symptoms, and speech and language development.”
The clinical delivery model of As You Are was developed to address these issues. Using validated diagnostic tools via telehealth addresses these issues in several ways, explained Dr. Hicks. “Virtual care can eliminate geographic barriers, making diagnostic resources available to more consumers with a shorter wait time. It can also provide more consumer convenience and direct-to-consumer services that eliminate the ‘need’ for a referral. And, when combined with a novel diagnostic aid like Autism Analytica, it can improve assessment accuracy and the quality of medical care.”
“The care coordination team is another big part of what we do,” said Dr. Hicks. “They work closely with families to implement the treatment plan created by the family and the As You Are physician. The care coordinators can identify speech therapists, occupational therapists, or ABA (Applied Behavioral Analysis) therapists in the family’s area and get those services started as soon as possible.”
Since 2022, As You Are has completed over 4,000 initial appointments. Patients seen by As You Are wait an average of three weeks for an appointment, as opposed to the nearly 12 month wait they faced prior to their As You Are referral. This dramatic reduction in wait times leads to earlier diagnoses, earlier intervention, and improved developmental outcomes for children with autism spectrum disorder.
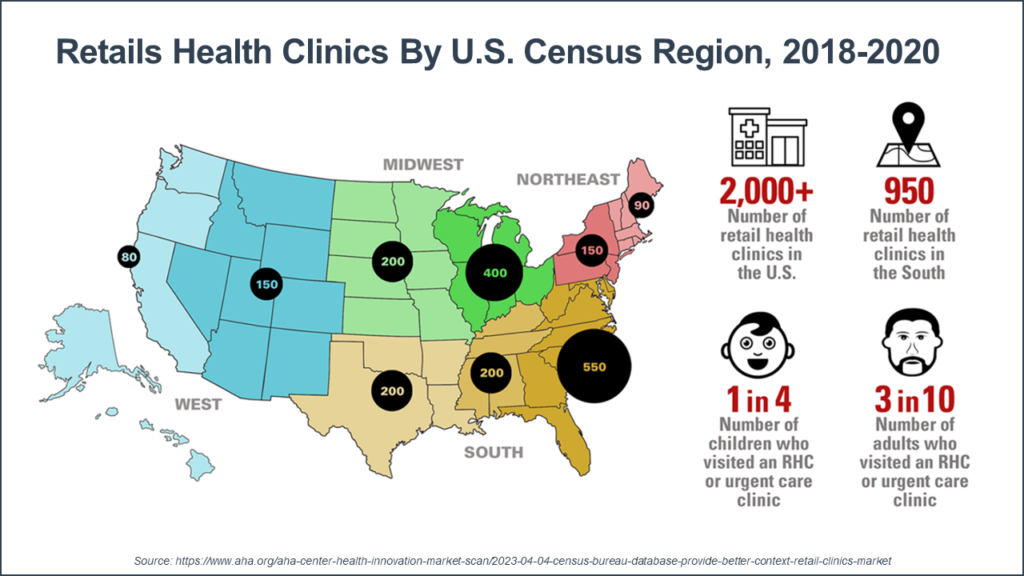
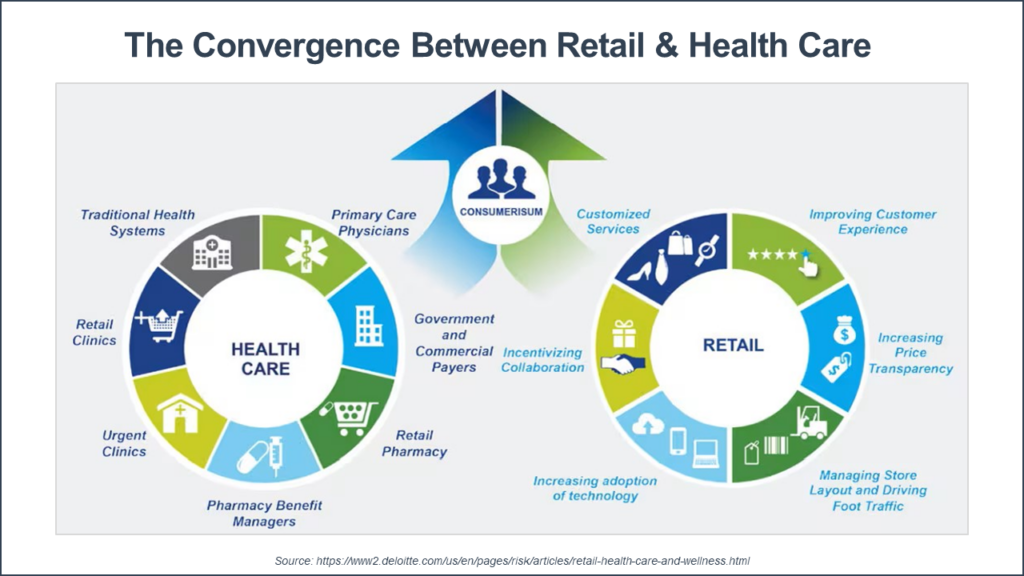
After last week, the trajectory of ‘convenient care’ sector of the health care field is becoming more clear. (By definition, convenient care are the services of companies and health care systems that provide consumers with accessible, affordable, quality health services in retail-based locations.) After the announcements of the past week, the footprint is expanding both in geography and service offerings.
One big development is the announcement last week by CVS that they will be expanding the services of Oak Street Clinics to 25 states from 21 by the end of this year—adding 50 to 60 new clinics. Oak Street currently employs about 600 primary care clinicians and has more than 170 medical centers (see CVS To Build More Than 50 Oak Street Senior Clinics In 2024). Many of the new Oak Street Clinic locations will be co-located with one of the 9,000+ CVS pharmacies and added to their 1,180 MinuteClinic locations.
And just this morning, Walmart announced their new relationship with the Association For Entrepreneurship USA, making a capitated no-deductible plan for primary care available to its 200,000 members. These services are part of a bundle with a PBM, a vision plan, group life insurance, and other benefits. The bundle fee is $19.97 per month for an individual and $29.95 for family coverage (see AFEUSA Selects Walmart Health to Offer Primary and Acute Care for $19.97 per Month!).
These developments are important in a few ways. Traditional provider organizations will need to strengthen their niche (and find new niches) serving consumers with more complex conditions. They are likely to lose market share and revenue for consumers who are not in the high-needs complex cohort (the 20% of the population using 80% of health care resources)—and need to build that revenue.
The opportunity is that primary care programs—and care coordination initiatives—for consumers with behavioral and cognitive challenges remain difficult to find—even with this expansion by the convenient care giants. And the Centers for Medicare and Medicaid Services (CMS) has opened up the window for using Medicare and Medicaid funds to pay for targeted social support programs and for services in correctional settings (see You Need Your Zs and Reaching In)—another new opportunity with this consumer population.
Another issue is that traditional provider organization executives cannot assume that most consumers in their community are “theirs” without sharpening their service offerings. There are new market entrants in serving this complex population—behavioral health urgent care centers and primary/behavioral integrated care for consumers with serious mental illnesses and intellectual disabilities. These new entrants are offering what payers and consumers are looking for—prompt access, hybrid service delivery, whole person approaches, a great experience, performance data, and reimbursement with financial risk.
The expansion of the health care services in retail locations is reshaping what payers expect (employers, Medicare plans, Medicaid plans); health plan contracting; and consumer options. Every organization in the health and human service field will need to consider the impact—and adjust their plans for sustainability and growth accordingly.
For more on the developments in convenient care, check out these resources in the OPEN MINDS Industry Library:
The challenge for managers of health and human service organizations is making hybrid health care services work for consumers and clinicians. This is no small feat because clinician and consumer preferences don’t necessarily align.
Consumers strongly prefer in-person visits, according to a soon-to-be-released survey from Ernst & Young (see Sneak Peek: New EY Survey Explores Changing Consumer Telehealth Preferences). Close to three in four (71%) consider the quality of in-person care is superior to that of virtual care. And while 44% of consumers would consider virtual primary care consultations, only 12% were willing to use virtual consultants for chronic conditions. Those findings are consistent with the drop in use of telehealth—5.5% of claims in February 2023, a drop of 6.8% from January (see Telehealth Declined Nationally In February, Fair Health Finds). Mental health remained the top telehealth diagnosis.
But the U.S. workforce in general—and clinicians specifically—would prefer to work virtually from home. A February 2022 survey found that 83% of workers prefer a hybrid model that lets them work remotely at least 25% of the time (see Work In Progress: How The Future Of Work Depends On Us). And Zip Recruiter data collected from each month in 2022 shows that 60% of job seekers are looking for remote work, with 20% saying they will not accept a position with any in-office work requirements (see Remote Work: A Win-Win-Win For Employees, Employers, And The Economy).
The question for managers is how to address workforce recruitment, retention, and productivity in this shifting employment market. That was the focus of the recent OPEN MINDS Circle Executive Roundtable, Maximizing Productivity In A Mixed Use Workforce — The Southwest Behavioral & Health Services Case Study, featuring Steven Sheets, President and Chief Executive Officer of Southwest Behavioral & Health Services (Southwest Behavioral) in Phoenix. Southwest Behavioral runs 16 outpatient clinics for consumers with serious mental illness, addictions, and HIV, with an annual revenue of $89 million. Southwest Behavioral delivers approximately 16,500 virtual services per month and 200,000 per year. And out of approximately 1,200 employees, 450 work in a hybrid arrangement.
“It’s important to understand the potential benefits and downfalls of different workplace scenarios,” Mr. Sheets explained. “The good—quick access to care and high-quality services that reach a lot of individuals The bad—some staff don’t want to come back to the office, even though many consumers want to be seen in person. And some teams just don’t function remotely as well, like our finance team, where critical communication with internal colleagues and external vendors suffered with remote and hybrid models.”
To address the issues of performance and productivity and make decisions about hybrid and remote work, Mr. Sheets recommends building a set of metrics that show where hybrid and remote work is working—in order to make decisions about who can work remotely and who needs to work in the office. It all starts with identifying the key performance indicators (KPIs)—quantifiable measures used to track progress toward achieving performance objectives. These KPIs can be reported by staff members, teams, and/or larger business units.
“It may take a lot of manpower and time to determine what you want to measure and how, but the investment here is critical,” said Mr. Sheets. “We pulled all the data from electronic health records and clearinghouse and mapped it all together so that we could create a dashboard tool to help us identify high- and low-performing clinical sites and teams. Clear metrics and measurement protocols are essential before you can reliably say if someone, or a group, is successful or not.”
These data allow managers to identify what people and what teams are under-performing and how that performance will affect team workflow and service delivery quality. But it’s just the first step. Context matters. according to Mr. Sheets. Why are they (or aren’t they) meeting expectations? What could be done to help improve performance? Executives need this information to have conversations with employees, to see the full picture and make staffing decisions accordingly. Things to look out for: employees may not have a conducive work environment at home; they may struggle using technology; or operational workflows may not adequately support the employee’s job.
To track performance, the Southwest Behavioral team uses a number of measures. For direct care staff, the measures include productivity (revenue benchmarking), quality metrics (no-show rates, timeliness of notes entered), and outcome measures (number of support sessions provided, length of stay). For administrative staff, these metrics include IT tickets addressed (response time and resolution time), billable services submitted for reimbursement (dollar amount of services submitted), and invoices paid.
“The key for us was to get buy-in from that staff and keep the lines of communication open,” said Mr. Sheets. “We believe that we have been able to manage a complex work force in a way where communication is the root of all that we do. Opening lines of communication is extremely important. More communication is better than less, even if it’s redundant. That makes the staff feel both engaged and that they have a seat at the table.”
The pandemic has increased consumer expectations to have the option for virtual services—but it has not greatly decreased the demand for face-to-face sessions. Executive teams need to develop a consumer-driven delivery system that provides services based on consumer preferences. This means creating the model with the processes, technology, and staff ready for this new reality.
For more guidance on remote and hybrid staffing, check out these resources in the OPEN MINDS Industry Library:
And for an in-depth look, join us June 14 for The 2023 OPEN MINDS Strategy & Innovation Institute session, The Tech & Human Infrastructure For Hybrid Care: Coordinating Virtual, In-Clinic & In-Home Services, featuring Doug Wright, Ph.D., Chief Operations Officer at Southeast Kansas Mental Health Center, and Shawna Wright, Ph.D., Director at the University of Kansas Center For Telemedicine & Telehealth.
One of the questions for specialty and primary care provider organization executive teams is how to participate in integrated systems of care. There are a variety of models—and no right answer. Some specialty provider organizations have added primary care services (see The Behaviorally-Led Primary Care Practice: Addressing Six Key Elements For Successful Integration), and some primary care organizations have added behavioral health clinicians to their clinical team. This integrated service delivery approach is the apparent future path of large insurers, such as CVS/Aenta acquiring Oak Street Health and Amazon’s acquisition of OneMedical.
As the white paper points out, combining data from disparate sources including physical health, behavioral health, and social determinants of health (SDOH) continues to be a challenge for providers. In the survey, 53% of respondents indicated that they are using existing operational technology to collect all the information they need. About 20% reported that they are using two separate systems, such as one for health records and another for collecting information such as SDOH referrals. Meanwhile 18% said they are using more than two systems. Lastly, 8% stated their technology use does not fit into any of those categories with one respondent describing they have had to move back to using paper models due to various issues with technology integration and implementation.
When asked about their upcoming technology functionality needs, coding topped the list. 65% of executives reporting needed better functionality for coding—particularly ICD-10 Z code for mental health. The next functionality lift has to do with incorporating consumer screening and assessment information into the EHR—26% reported needing functionality for SDOH screening questions and 17% for consumer assessments. 22% were looking for integration of consumer survey data into the EHR. And, 19% were looking for functionality to support SDOH initiatives.
The focus on social determinants and consumer input is not surprising with the shift to a whole person care models—and the increased integration of performance-based measures in reimbursement. For success, provider organizations need to ‘manage’ medical, behavioral, and social services—even if they are not providing those services. And, the most common performance metrics—ER use, readmissions, HEDIS, and CMS Stars—all lean heavily on consumer experience and consumer engagement.
The push to integrated care models and whole person care approaches to service delivery is continuing. The challenge is that every payer—and every health plan—has a slightly different model for making integration happen. In the year ahead, we have planned a number of sessions focused on the payer and health plan perspectives on “best practice” integration strategies:
For even more on integration, mark your calendar for June 15 in New Orleans at The 2023 OPEN MINDS Strategy & Innovation Institute and for the session, Integrating Digital Tools Into Service Delivery, featuring Stephen Smith, Cofounder and Chief Executive Officer for NOCD.